It is generally accepted that reported / known COVID-19 cases represent only a fraction of real cases; we continue to adopt a figure of about 22% known cases cumulatively for the outbreak as a whole. Reported case numbers also depend on the criteria for testing, the volume of tests, the time taken to produce a test result and test accuracy; all of these factors are in flux to some degree in most regions. However known case data remains the best information that we have to assess the state of the outbreak and we continue to use those data in the models today.
Our model 3 (available
here) tracks the population and predicts the numbers who have been exposed, infected, isolated and cured; it combines the (testing) time lag of detection relative to infection that we used in
model 1, with the 22% cumulative detection rate we used in
model 2 and represents a small evolution that we think improves it's correspondence with reality. We see this as a fit for purpose model and future postings are unlikely to change the model much, only to apply it to the latest data.
Results to date and projected to the end of 2020 are summarized below for Ireland, Italy and the United States. Projections support the view that the month of April may see a peak in demand for ICU beds in each of those regions if the current restrictions are maintained and observed by the public. Note that in each case, the estimated number of ICU beds needed is based on the number of known cases currently in isolation and assumes that 5% of those require an ICU bed.
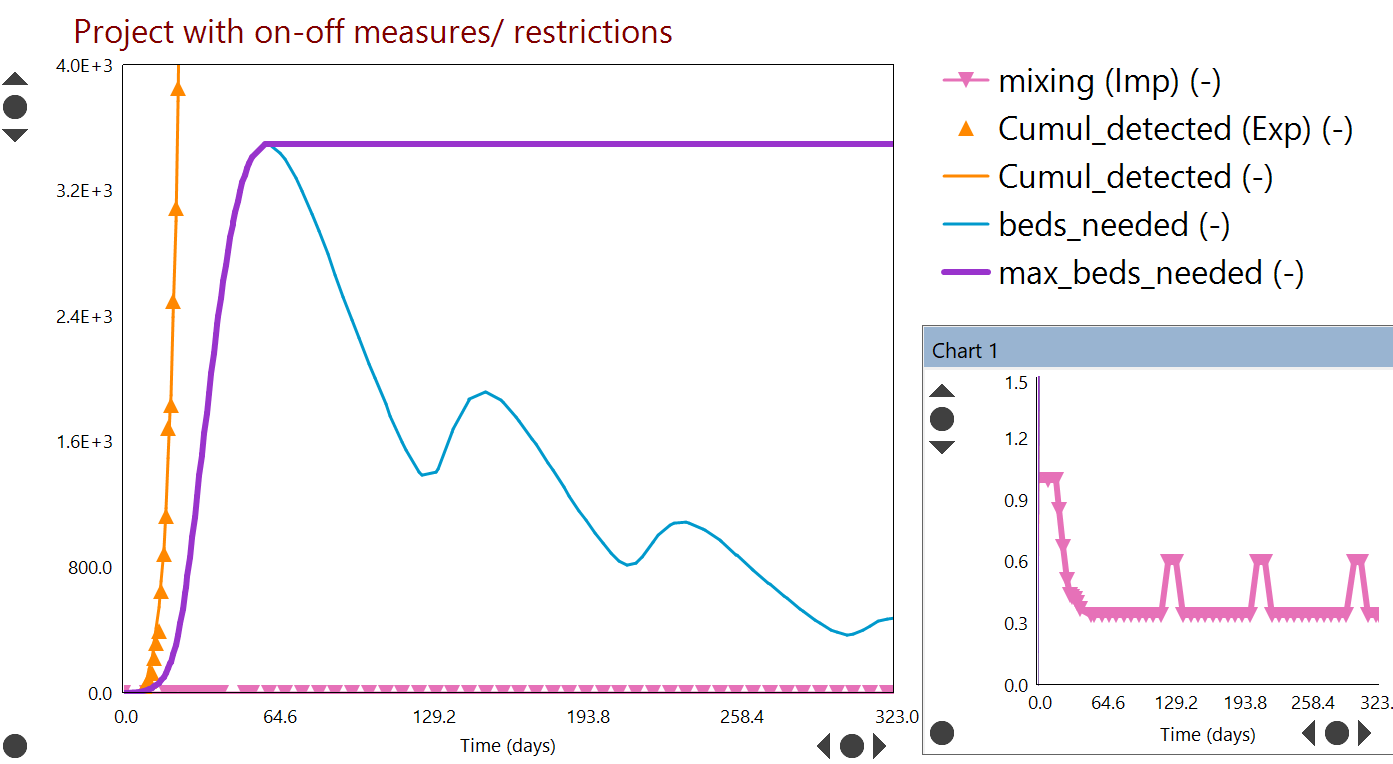
The question of how to emerge from the pandemic is difficult, with indications that general restrictions similar to those currently in place cannot be relaxed much for the foreseeable future. As usual in the plots, discrete symbols like 🔺indicate measured / real reported case data (denoted in the legend as 'Exp' for 'experimentally measured') and curves indicate model predictions. When curves pass through symbols of the same colour, the model agrees well with measured data. The 'mixing' variable [inset] is an indicator of the extent of people movement, with 1.0 as the base case (before restrictions) and lower values after restrictions have taken effect.
Ireland:
 |
| Ireland: If current restrictions remain in place [inset] and are observed by the public, the model suggests that peak ICU demand will be reached around day 63, between 20-27 April. Relaxation of restrictions [inset] will lead to further peaks later in the year. |
Italy:
 |
| Italy: If current restrictions remain in place [inset] and are observed by the public, the model suggests that peak ICU demand will be reached near day 61, around 13 April. Relaxation of restrictions [inset] will lead to further peaks later in the year. |
Unites States (as a whole):
 |
| United States: If current restrictions remain in place [inset] and are observed by the public, the model suggests that peak ICU demand will be reached around day 93, between 20-27 April. Relaxation of restrictions [inset] will lead to further peaks later in the year. |


No comments:
Post a Comment